



If there is 50+ causes of heel pain, how do I treat it?
Posted on 3rd February 2020 at 11:32
Recently I treated a new patient who had been diagnosed with Plantar Fasciitis by her G.P. weeks ago and had been hobbling round ever since in agony.
A podiatrist who treats heel pain will never have a chat and hand you a pair of insoles.
I take about an hour. In this time, I take a medical and family history. This is to understand if there are any underlying conditions that you already know of that may contribute to the problem, medications that you take that may interfere with treatment or anything that you may not have flagged up that may affect diagnose or treatment.
Next, I carry out a clinical examination. In this I look and the hip, knee and feet in detail as well as the leg as a whole, I also look at the pelvis, shoulders, arms and head. This is done non-weightbearing and weightbearing and I am looking for irregularities and asymmetry as well as muscle and bony blocks or neurological issues that a affect you.
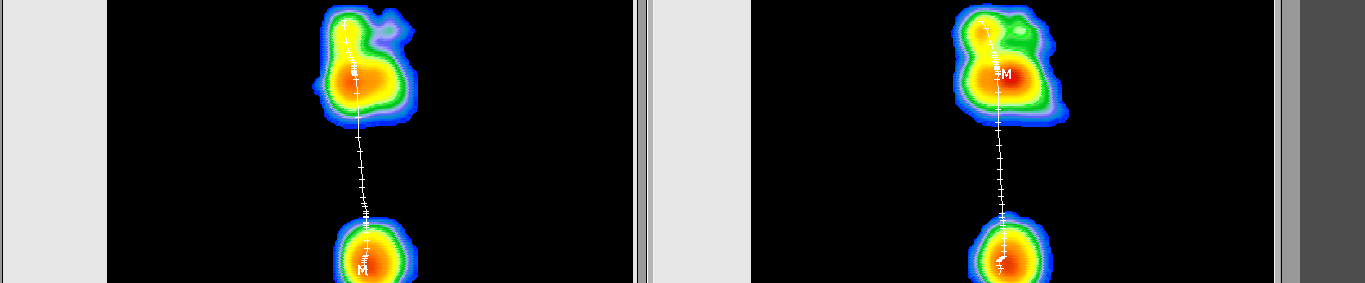
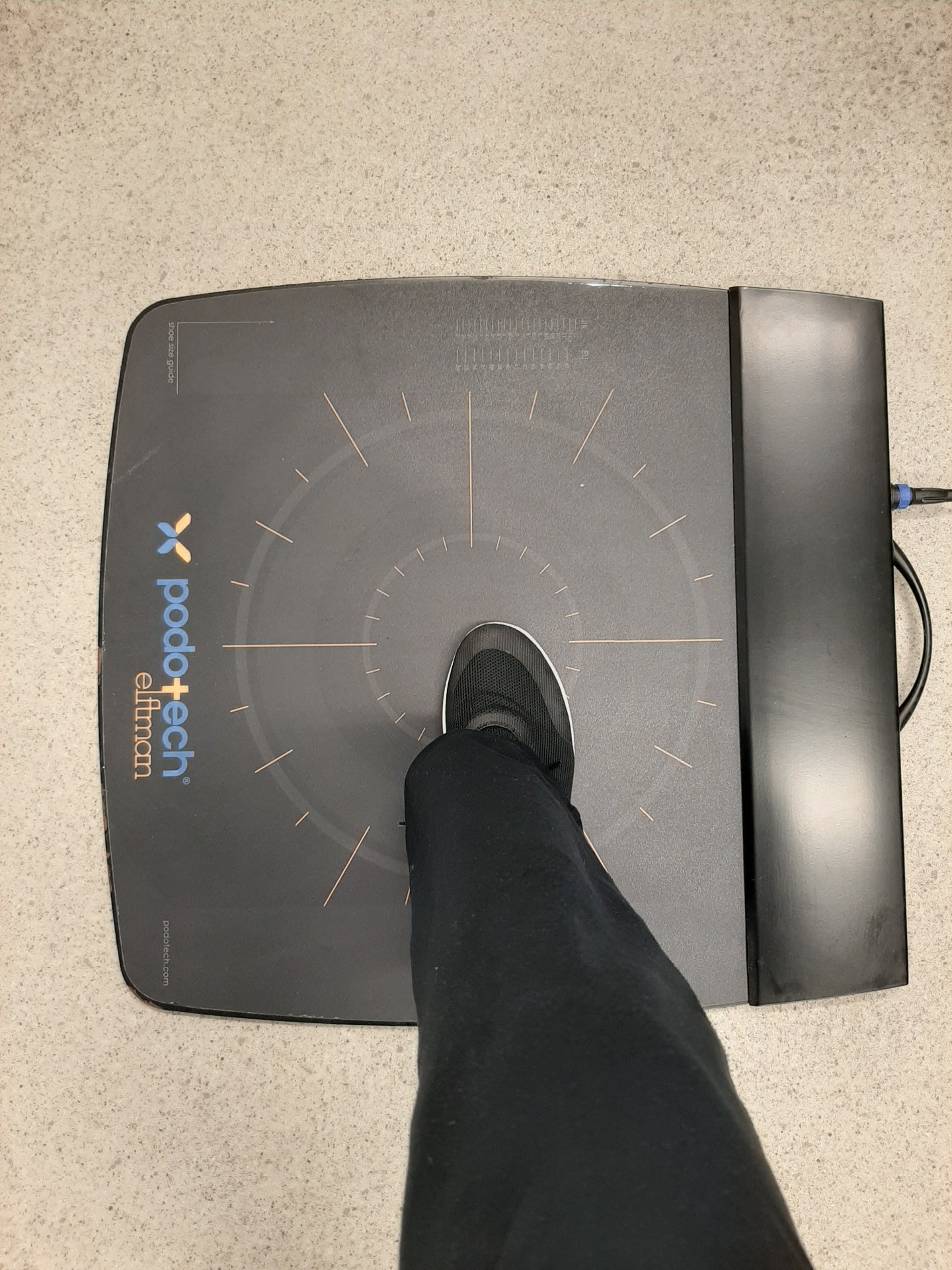
The dynamic assessment consists of gait captured on slow motion cameras and pressure plates to assist in diagnosis and help patient comprehension as well as allowing me to store this data for comparison in future visits.
All this allows me to build up a picture of how you walk, run, carry out activities and chip away at differential diagnoses to filter out the likely causes. Sometimes I will need to refer you for an Xray, Ultrasound or MRI to help me to come the correct diagnosis and this also ensures that I don’t jump into an incorrect treatment that may in fact exacerbate your heel pain.
Often, I am able to embark on a short-term treatment to assist you through the early stages of healing. Don’t forget that it will have taken you some time to get from initial pain to my clinic and I do not have a magic wand to wave that will instantly reverse this. Most of the most common causes of heel pain are, in short, repetitive strain injuries and treatment will reflect this. Acute treatments include, rest and ice, strapping to support the affected tissues, controlling the pain cycle through oral medication and possibly some minor intervention such as a heel raise. Footwear advise is often part of this stage.
Longer term treatments will be prescribed depending on the cause of your heel pain and the likely success of these treatments on that cause. Rehabilitation Exercises, Weight Loss, Orthoses, Corticosteroid Injections, Dermal Fillers and Shockwave Therapy are often used in isolation or conjunction and, again, this depends on many factors. Occasionally a surgical referral is necessary.
I often use a questionnaire call the ‘Foot Function Index’ to help me to record the patient’s pain, activities and quality of life at day one of treatment and then again six to eight weeks after intervention. Our perspective of pain etc can be hard to quantify without such a tool and this helps the patient realise how far they have come.
I find that the secret to a successful long-term treatment is, really understanding the causative and exacerbatory factors and limiting exposure to these. Once symptoms are under control, a plan to prevent recurrence can be put in place and may be as simple as good footwear or daily stretches.
The patient I mentioned earlier on did not have plantar fasciitis but a fractured calcaneus (heel bone), she has osteoporosis and received the treatment she required through the fracture clinic as soon as I suspected a fracture by examining her heel, this was confirmed on X-ray. She is doing well.
Stride Clinic Help Heal Heel Pain using the 3 P’s of Plantar Heel Pain
• Pain Diagnosis
• Plan Your Treatment
• Prevent Recurrence
Tagged as: Heel Pain, Plantar Fasciitis
Share this post: